

So lately I have seen more than a couple failed kick offs. Not necessarily on this forum but this is where I am calling home so this is where I will post this. Mostly there seems to be a confusion about half lives. So I figure I will share some medical knowledge to help out the brothers here.
Half lives:
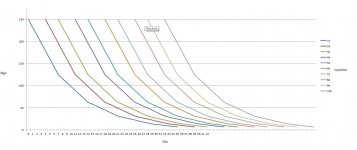
Every drug has a half-life. Half-life is the amount of time it will take for your body to use half of the drug. The other half still remains in your body. So if you have a drug with a seven day half-life and you take 250mgs of it, your body will use 125mgs in 7 days then you have another 125mgs left in your body. Your body will use half of that, 62.5, over the next seven days, leaving 62.5... and so on and so on. This continues until there is nothing left of the drug, and this can actually take a very long time. Which is why even though the half life may only be seven days the detection time may be much, much longer, but I will explain that below. This all leads to why people say you wont notice a test e cycle of 500mgs a week until week 5, as its during week 4 when your levels finally level/max out, this can be seen in the chart below. This also is the cause for shorter esters to kick in faster. The example of test prop, which has a 3 day half-life, will actually level/max out around day 15, also shown below. On each day, add together the amount of each line to give you the total amount in your system.
Kickoff:
So knowing what we know now we can see that even if we were to inject much more of the total amount of each drug into out system, the amounts could be lower than they would be somewhere later into our cycle. Meaning that you can inject 500mgs of test e a week into your system along with 350 of test prop a week and still not hit any extreme levels. This is actually how a proper kick off should be done, as it will allow your system to build up the proper amount by day 14 instead of day 30. This is shown in the chart below. The grey line indicates the total amount of test in your system.
Detection times:
Some drugs are also easier to detect than others. This is why nandrolone deconate has such a longer detection that test deconate. The esters are the same, but even though after a year maybe only .02mgs of each may be present, the nandrolone is the only one that is detectable. This is primarily due to nandrolone being a unnatural substance.
Active-life:
Forget this term, it will confuse you.
Prop chart: 150mgs eod, figured with a 3 day half-life
Enth chart: 250mgs every 3-4days, figured with a 7 day half-life, even though some say it may be as long as 10 days.
Kickoff chart: it may look confuseing but it is test prop injected 100mgs eod and test e at 250mgs every 3-4 days. The grey line at the topis the total amount in your system.
I have tried to explain this as simple as I can, I hope this helps someone!
T
other charts in next posts
Half lives:
Every drug has a half-life. Half-life is the amount of time it will take for your body to use half of the drug. The other half still remains in your body. So if you have a drug with a seven day half-life and you take 250mgs of it, your body will use 125mgs in 7 days then you have another 125mgs left in your body. Your body will use half of that, 62.5, over the next seven days, leaving 62.5... and so on and so on. This continues until there is nothing left of the drug, and this can actually take a very long time. Which is why even though the half life may only be seven days the detection time may be much, much longer, but I will explain that below. This all leads to why people say you wont notice a test e cycle of 500mgs a week until week 5, as its during week 4 when your levels finally level/max out, this can be seen in the chart below. This also is the cause for shorter esters to kick in faster. The example of test prop, which has a 3 day half-life, will actually level/max out around day 15, also shown below. On each day, add together the amount of each line to give you the total amount in your system.
Kickoff:
So knowing what we know now we can see that even if we were to inject much more of the total amount of each drug into out system, the amounts could be lower than they would be somewhere later into our cycle. Meaning that you can inject 500mgs of test e a week into your system along with 350 of test prop a week and still not hit any extreme levels. This is actually how a proper kick off should be done, as it will allow your system to build up the proper amount by day 14 instead of day 30. This is shown in the chart below. The grey line indicates the total amount of test in your system.
Detection times:
Some drugs are also easier to detect than others. This is why nandrolone deconate has such a longer detection that test deconate. The esters are the same, but even though after a year maybe only .02mgs of each may be present, the nandrolone is the only one that is detectable. This is primarily due to nandrolone being a unnatural substance.
Active-life:
Forget this term, it will confuse you.
Prop chart: 150mgs eod, figured with a 3 day half-life
Enth chart: 250mgs every 3-4days, figured with a 7 day half-life, even though some say it may be as long as 10 days.
Kickoff chart: it may look confuseing but it is test prop injected 100mgs eod and test e at 250mgs every 3-4 days. The grey line at the topis the total amount in your system.
I have tried to explain this as simple as I can, I hope this helps someone!
T
other charts in next posts



")



